At the Centeno-Schultz Clinic we acknowledge that shoulder pain can compromise quality of life and athletic endeavors.
Our online book, Ortho 2.0 highlights a systemic evaluation of joint pain and dysfunction. The approach is termed SANS.
The N is SANS denotes nerve dysfunction.
Axillary nerve dysfunction can be a cause of lateral arm numbness and shoulder weakness.
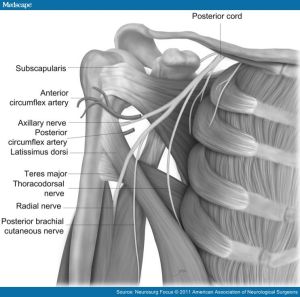
The Axillary nerve arises from the posterior cord of the brachial plexus, C5 and C6.
Course: It crosses the antero-inferior aspect of the subscapularis muscle, passes behind the arm through the quadrilateral space, winding around the neck of the humerus ending in two major trunks: anterior and posterior trunk.
Innervation: Teres Minor and Deltoid
Sensory: Lateral deltoid also known as the regimental badge area.

Injury can occur at several sites along the nerve path:
Origin of the posterior cord
Anterior-inferior aspect of the subscapularis muscle
Quadrilateral Space:
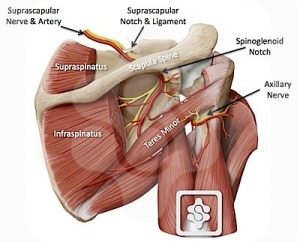
The quadrilateral space is bounded superiorly by the teres minor muscle, inferiorly by the teres major muscle, medially by the long head of the triceps, and laterally by the humeral shaft.
Common presentation is dull intermittent ache or pain that is localized in the posterior and lateral shoulder. Symptoms are exacerbated by active and resisted abduction and external rotation of the humerus.
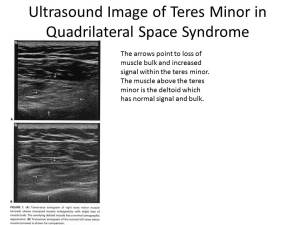
Quadrilateral space syndrome is an affliction of middle-aged men and it presents classically in the throwing athlete and those with a history rotator cuff surgery.
Ultrasound examination is can be significant for atrophy of the teres minor muscle which is illustrated below.
injury at several sitesgin from the posterior cordAnteroinferior aspect of the subscapularis muscle and shoulder capsuleQuadrilateral space